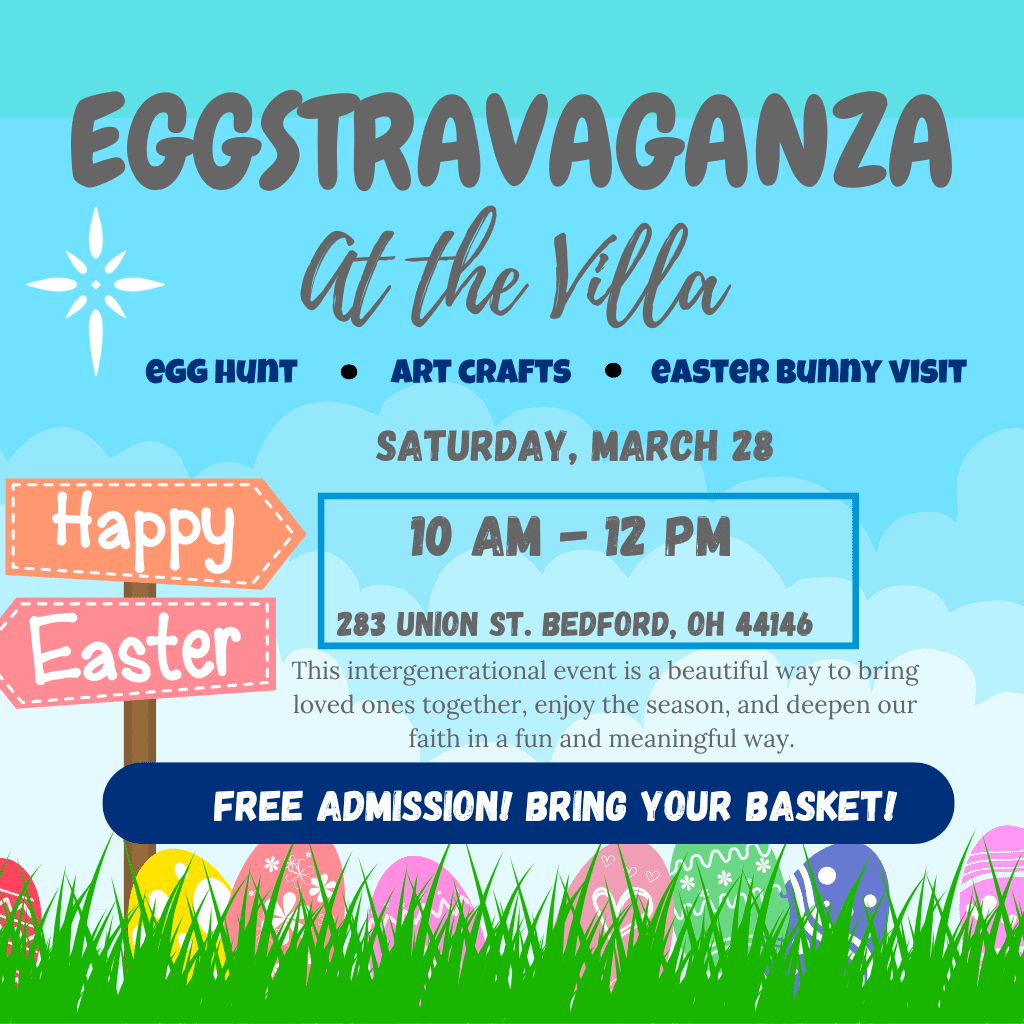
Eggstravaganza at the Villa!
On Saturday, March 28 at 10 AM, families and friends are invited to bring their little ones for an Easter Egg Hunt across the Villa!










On Saturday, March 28 at 10 AM, families and friends are invited to bring their little ones for an Easter Egg Hunt across the Villa!
As we celebrate the 175th Anniversary of the Sisters of Charity of St. Augustine, we invite you to join us for a special afternoon of prayer and gratitude on Wednesday, April 29.

We are thrilled to share exciting news with our community — Light of Hearts Villa has officially received a deficiency-free rating on our 2025 Annual State Survey conducted by the Ohio Department of Health!